How personalised DBS surgery, expert diagnosis, and a decade-seasoned multidisciplinary team at Jaslok Hospital deliver outcomes that go far beyond motor control.
Dr. Paresh Doshi | Director of Stereotactic and Functional Neurosurgery and Director of Neurosurgery, Jaslok Hospital, Mumbai

KEY TAKEAWAYS FROM THIS ARTICLE
What determines the success rate in Deep Brain Stimulation surgery?
✔ Correct diagnosis is the single most important prerequisite
Misdiagnosed Parkinson’s disease — particularly Parkinsonism-plus syndromes mistaken for idiopathic PD — is the leading cause of DBS failure worldwide. Clinical expertise in differential diagnosis is not optional; it is the foundation on which all surgical success is built.
✔ DBS must be personalised to each patient’s disease profile and life
With multiple device types, targets, and stimulation strategies now available, DBS is no longer a single operation — it is a personalised prescription. The surgeon’s understanding of who the patient is — their work, their priorities, their disease subtype — determines which surgery they should have and what success means for them.
✔ Success is quality of life — not just motor scores
UPDRS motor scores are a measurement tool. Quality of life is the goal. A patient who walks better but develops untreated depression or unmanaged cognitive decline has not been successfully treated. True DBS success requires tracking and managing the full spectrum of Parkinson’s disease — motor and non-motor alike.
✔ A multidisciplinary team with 10–15 years of shared experience is irreplaceable
The accumulated institutional knowledge of a mature MDT — neurologist, neurosurgeon, neurophysiologist, neuropsychologist, programmer, and rehabilitation specialist working together across hundreds of patients over more than a decade — cannot be replicated quickly or approximated. This is the Jaslok Hospital difference.
When patients and families ask about the success rate of Deep Brain Stimulation surgery, they are rarely asking about UPDRS motor scores or tremor amplitude measurements. They are asking something far more human: Will I get my life back? Will I be able to do the things that matter to me? Will I feel like myself again?
At Jaslok Hospital, we have been answering that question for over two decades — and our answer has grown more sophisticated, more personalised, and more complete with every passing year. Success in DBS surgery is not a single number. It is not the percentage reduction in “off” time, nor the improvement in a standardised rating scale. It is the convergence of the right diagnosis, the right surgical strategy for the right patient, flawlessly executed, and followed by years of expert, coordinated care. Each of these elements is essential. The absence of any one of them can turn a technically perfect operation into a clinical disappointment.
The most underappreciated cause of DBS “failure” is not surgical error, hardware malfunction, or poor programming. It is something that happens long before the patient ever reaches the operating theatre: a wrong diagnosis.
Parkinson’s disease is the most common movement disorder referred for DBS surgery — but it is also one of the most frequently misdiagnosed conditions in neurology. Population-based pathological studies have consistently shown that up to 20–25% of patients clinically diagnosed with Parkinson’s disease during life do not, in fact, have idiopathic Parkinson’s disease at autopsy. They have Parkinsonism-plus syndromes — Progressive Supranuclear Palsy (PSP), Multiple System Atrophy (MSA), Corticobasal Degeneration (CBD), Dementia with Lewy Bodies, or Vascular Parkinsonism — conditions that look like Parkinson’s disease in their early stages but do not respond to DBS and, in some cases, may be worsened by it.
This is not a peripheral concern. It is the central clinical challenge of DBS surgery. A patient with PSP who undergoes subthalamic nucleus DBS will not improve. They may deteriorate. The surgery will be labelled a failure. But the surgery was never the problem — the diagnosis was.
At Jaslok Hospital, the rigour of our pre-operative diagnostic workup is the foundation of our outcomes. Every patient referred for DBS assessment undergoes a structured process that includes long-term clinical observation, response to levodopa challenge, detailed neuroimaging review including DaTscan where indicated, and multidisciplinary consensus before any surgical recommendation is made. The years of experience our neurological team brings to this process — pattern recognition refined across hundreds of cases — is something that cannot be taught from a textbook and cannot be acquired rapidly.
Parkinson’s disease is not one condition. It is a family of conditions that share a name, a pathological hallmark (alpha-synuclein aggregation), and a broad set of motor features — but differ profoundly in their molecular drivers, their clinical trajectories, their non-motor profiles, and their responses to treatment. The era of personalised DBS has arrived, and at Jaslok Hospital, we have been practising it long before the term became fashionable
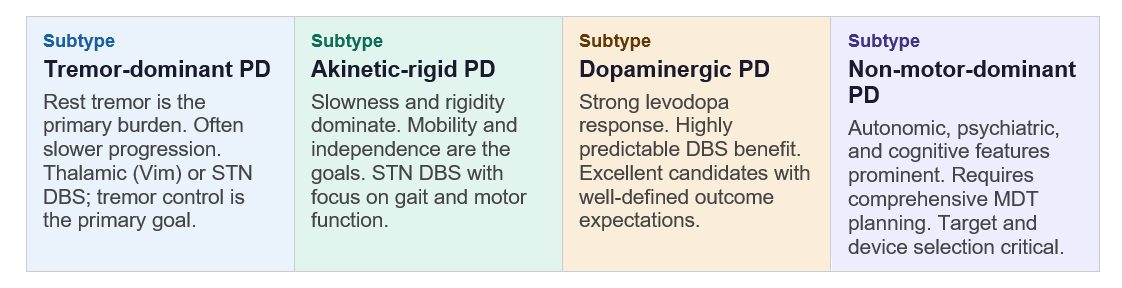
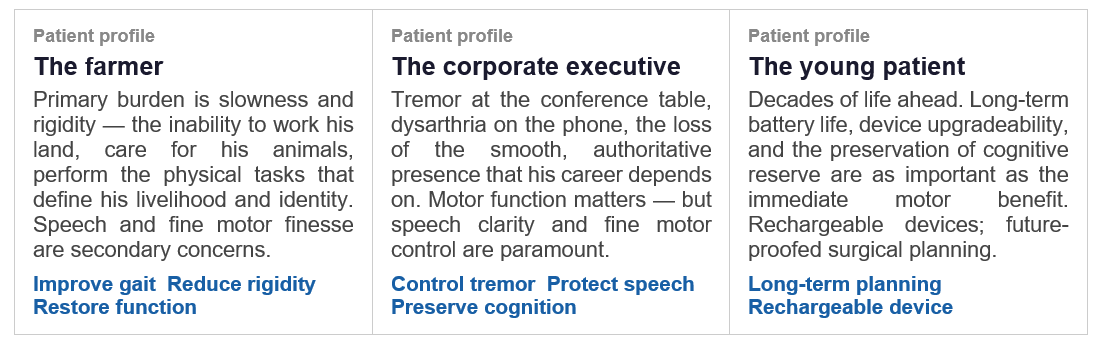
Beyond disease subtype, the patient’s life context is inseparable from the surgical plan. Two patients with identical UPDRS scores and identical MRI findings may need fundamentally different surgeries because their definition of success is fundamentally different.
This level of personalisation — matching device type, stimulation target, surgical approach, and outcome priorities to the individual patient — is only possible when the clinical team has seen enough cases, in enough depth, over enough time, to know which variables matter and how they interact. It is the product of experience that cannot be compressed.
The long-term outcomes literature for DBS surgery in Parkinson’s disease is now mature and consistent. Our programme at Jaslok Hospital has contributed to this evidence base through peer-reviewed publications tracking patients across years and decades of follow-up — studies that capture not just what happens at three or six months, but what DBS truly delivers across the arc of a patient’s life with Parkinson’s disease.
Long-term motor outcomes of STN-DBS in Parkinson’s disease: 5-year resultsFive-year follow-up data from our series demonstrating sustained motor benefit, reduced off-time, and significant improvement in activities of daily living in patients with Parkinson’s disease treated with subthalamic nucleus DBS at Jaslok Hospital, Mumbai. ✔ Sustained motor benefit at 5 years |
Ten-year longitudinal follow-up data tracking motor function, quality of life scales, medication requirements, and non-motor outcomes in patients with Parkinson’s disease who underwent DBS surgery at our centre. This study captures the full trajectory of DBS benefit and its evolution alongside disease progression.
The paper goes on to conclude: STN-DBS provided sustained motor improvement, with tremor and rigidity showing the most significant benefits after 10 years. The initial 3 years likely represented a “DBS honeymoon,” with peak improvements in motor and nonmotor symptoms. Genotype may influence the efficacy of DBS, and monitoring rare complications is essential.
✔ QoL and motor outcomes at 10 years
Across both short- and long-term follow-up, the data from our programme aligns with the best international centres: approximately 50–60% reduction in “off” time, 40–60% improvement in UPDRS-III motor scores in the “off” state, and significant reductions in levodopa-equivalent daily dose. But the numbers that matter most to patients — the return to meaningful activity, the restoration of independence, the re-entry into social and professional life — are the ones that motivate our team every day.
The conventional success metrics of DBS surgery — UPDRS-III, timed tests, dyskinesia scales — measure the motor domain of Parkinson’s disease. But Parkinson’s disease is not a motor disease with some non-motor features. It is a whole-body, whole-brain condition whose impact on quality of life is driven by a complex web of symptoms that extend far beyond movement.
A patient with excellent motor control after DBS surgery who has untreated cognitive decline, unmanaged bladder dysfunction, chronic neuropathic pain, or significant depression is not a DBS success story. They are a patient who received a motor treatment for a disease that needed comprehensive treatment. The distinction is not semantic — it is the difference between a technically successful operation and a clinically successful outcome for a whole person.
The non-motor domains that determine quality of life in Parkinson’s disease include:
● Cognitive function and dementia risk | ● Depression and anxiety disorders |
● Psychosis and impulse control | ● Bladder and urological dysfunction |
● Chronic pain and sensory disturbance | ● Sleep disorders and fatigue |
● Autonomic dysfunction | ● Speech and swallowing difficulties |
● Postural instability and falls | ● Social isolation and carer burden |
Each of these domains requires a specialist. Cognitive concerns require a neuropsychologist with deep familiarity with Parkinson’s disease. Bladder dysfunction requires a urologist integrated into the Parkinson’s care pathway. Chronic pain in Parkinson’s disease has unique characteristics that require a pain specialist who understands the dopaminergic underpinnings of central pain sensitisation.
A multidisciplinary team for DBS can be assembled on paper in a matter of months. What is extraordinarily difficult, and what takes a decade or more to build, is the shared clinical language, the accumulated institutional memory, the refined protocols born from hundreds of real cases, and the trust between team members that allows them to disagree productively when a patient’s management is genuinely uncertain.
NeurosurgeryDr. Paresh DoshiSurgical planning, electrode placement, hardware management, intraoperative neurophysiology oversight | NeurologyMovement Disorder NeurologistPre-operative diagnosis, candidate selection, levodopa optimisation, long-term disease monitoring | NeuropsychologyDBS NeuropsychologistCognitive baseline, surgical risk stratification, post-operative monitoring, psychiatric support |
ProgrammingDBS ProgrammerDevice optimisation, stimulation parameter refinement, troubleshooting, long-term programming strategy | NeurophysiologyIntraoperative SpecialistMicroelectrode recording, real-time target confirmation, awake patient monitoring during surgery | RehabilitationPhysiotherapy & SLTMotor rehabilitation, speech therapy, gait retraining, functional recovery optimisation |
At Jaslok Hospital, our MDT has been working together for over 15 years. In that time, we have developed clinical protocols that no textbook contains — protocols built from the cases that didn’t go as expected, the patients who improved in ways we didn’t predict, and the complications we learned to prevent through the hard work of honest self-reflection. This institutional knowledge lives not in any single member of the team, but in the team itself.
This is not something that can be built quickly. A programme that has been offering DBS surgery for three years, even with talented individuals, does not have this. It cannot have it. The knowledge requires the time, and the time requires the commitment to a single centre, a single team, and a single standard of care across every patient — which is precisely what the Jaslok Hospital DBS programme represents.
“The question is never whether DBS works. The evidence is overwhelming that it does. The question is whether the team performing it, and caring for the patient afterwards, has built the depth of expertise and the breadth of multidisciplinary capability to deliver not just a technically successful operation, but a genuinely transformed life.”
— Dr. Paresh Doshi, Jaslok Hospital, Mumbai
Success in DBS surgery at Jaslok Hospital is measured in the way that truly matters: in patients who return to work, who reconnect with their families, who recover the activities and relationships that Parkinson’s disease had taken from them. It is measured in patients who were correctly diagnosed when others had missed the signs of a misdiagnosed Parkinsonian syndrome. It is measured in the farmer who can tend his fields again, and in the executive who speaks at boardroom meetings without embarrassment. It is measured in the patients who, at five and ten years of follow-up, tell us that the surgery changed not just their movement but their lives.
That is what a personalised, multidisciplinary, experience-driven DBS programme delivers. And it is what we at Jaslok Hospital have spent two decades building — one patient, one surgery, one year of follow-up at a time.
About this article Dr. Paresh Doshi is a Director of Stereotactic and Functional Neurosurgery and Director of Neurosurgery, at Jaslok Hospital, Mumbai, with one of the largest DBS case volumes in Asia. His published research includes peer-reviewed studies on long-term DBS outcomes in Parkinson’s disease. This article is intended for patient education and does not constitute individual medical advice. |
Deep Brain Stimulation (DBS) is a highly effective treatment for Parkinson’s disease, with studies showing around 60–80% reduction in “off” time and 40–70% improvement in motor symptoms, leading to better movement, independence, and overall quality of life when performed with the right expertise. Its success depends on accurate diagnosis, a personalised surgical approach, and the support of an experienced multidisciplinary team, as seen at Jaslok Hospital. With proper patient selection and long-term care, many patients continue to experience meaningful benefits for 5–10 years or more, making DBS not just a procedure but a long-term treatment strategy focused on restoring everyday life.
Deep Brain Stimulation (DBS) surgery can significantly improve symptoms such as tremors, stiffness, slowness, and dyskinesia in appropriately selected Parkinson’s patients. Success rates vary depending on patient selection, disease stage, and surgical expertise.
No, DBS does not cure Parkinson’s disease. However, it can help manage symptoms effectively and improve quality of life for many patients.
Symptoms that commonly improve after DBS surgery include:
Results may vary from patient to patient.
Many patients experience long-term benefits from DBS surgery for several years. Regular follow-ups and programming adjustments help maintain symptom control.
Important factors include:
DBS surgery is generally considered safe when performed by an experienced neurosurgical team. As with any brain surgery, there are potential risks and complications which are discussed before treatment.
Patients who:
Yes, DBS is commonly used to help manage severe tremors associated with Parkinson’s disease and Essential Tremor when medications become less effective.
Most patients recover gradually over a few weeks. Device programming and symptom optimization continue after surgery through follow-up sessions.
Age alone does not determine eligibility for DBS surgery. Overall health condition, cognitive status, and neurological evaluation are important factors.
WhatsApp us