Medical management
- Initial management should be directed at the basics of airway, breathing and circulation.
- ICU admission and monitoring
- Frequent neurological examination
- Management of blood pressure
- Correction of underlying coagulopathies
- The routine use of steroids has not been shown to improve outcome
- Normalization of ICP which involves elevation of the head of bed, CSF drainage, pain medication and sedation, and osmotic therapy
- Anti-convulsant therapy
- Control of hyperglycemia
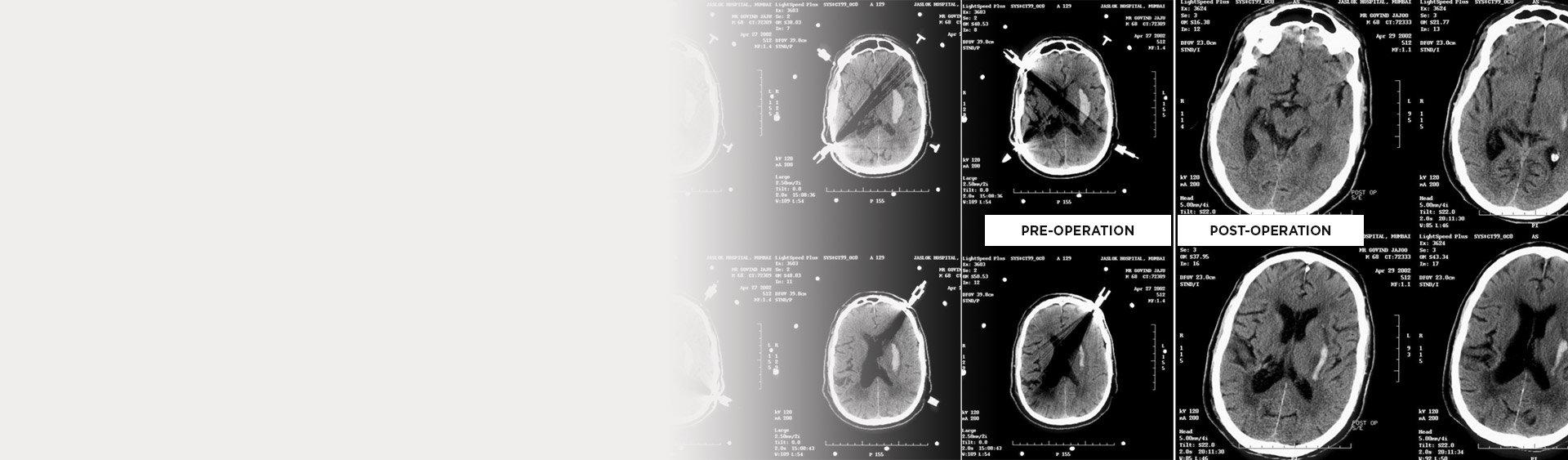
Stereotactic aspiration of intracranial bleed
Stereotactic evacuation of thalamic hematoma has improved survival rates as compared to craniotomy and evacuation.
Mortality following craniotomy was 34% versus 6.8% following stereotactic aspiration
Aim
- Relief of Intracranial hypertension
- Subtotal evacuation of the clot
- Avoidance of injury to important structures
Indications
- Volume >15ml. (> 3cm)
- Site: thalamic, putaminal, lobar
- Altered level of sensorium
- Neurological deficit
- Preferably within 72 hrs.
- Maximum duration – 4 weeks
- Surgically poor candidate who cannot tolerate anaesthesia.
Advantages
- Use of local anaesthesia
- Shorter operating time
- Less damage to surrounding normal brain.
- Allows complete hematoma removal
- Provide means for improved haemostasis
Contraindications
- Deeply comatose
- Signs of herniation – dilated pupil, decerebration
- Short life expectancy
- AVM & Aneurysm