Primary immediate effect
- Hemorrhage growth
- Increase ICP
Secondary effect
- Downstream effect
- Oedema
- Ischemia
Plausible mechanisms of neurological deterioration following development of
Perihaematomal oedemas are:
(1) Mass effect introduced by perihaematomal edema on an already challenged intracranial compliance.
(2) Secondary neuronal injury triggered by blood/degradation products (“hemotoxicity”) with potential to alter brain function.
Removal of the clot may diminish secondary tissue destruction and edema in the vicinity of the hematoma, either by preventing compartmental pressure changes and consecutive reduction of the blood flow perfusion pressure or by removing the changes caused by toxic blood byproducts. Fibrinolysis aids rapid dissolution of the remaining blood. The aim is to achieve a mass reduction as well as to reduce the extension of perifocal edema and minimize the amount of tissue damage. A urokinase washout can be performed for up to 7 days after the bleeding.
Sites of bleed
- basal ganglia (40-50%),
- lobar regions (20-50%),
- thalamus (10-15%),
- pons (5-12%),
- cerebellum (5-10%),
- other brainstem sites (1-5%).
Clinical presentation
- Alteration in level of consciousness (approximately 50%)
- Nausea and vomiting (approximately 40-50%)
- Headache (approximately 40%)
- Seizures [3] (approximately 6-7%)
- Focal neurological deficits
Focal neurological deficits
- Putamen – Contralateral hemiparesis, contralateral sensory loss, contralateral conjugate gaze paresis, homonymous hemianopia, aphasia, neglect, or apraxia
- Thalamus – Contralateral sensory loss, contralateral hemiparesis, gaze paresis, homonymous hemianopia, miosis, aphasia, or confusion
- Lobar – Contralateral hemiparesis or sensory loss, contralateral conjugate gaze paresis, homonymous hemianopia, abulia, aphasia, neglect, or apraxia
- Caudate nucleus – Contralateral hemiparesis, contralateral conjugate gaze paresis, or confusion
- Brain stem – Quadriparesis, facial weakness, decreased level of consciousness, gaze paresis, ocular bobbing, miosis, or autonomic instability
- Cerebellum – Ataxia, usually beginning in the trunk, ipsilateral facial weakness, ipsilateral sensory loss, gaze paresis, skew deviation, miosis, or decreased level of consciousness
Investigations
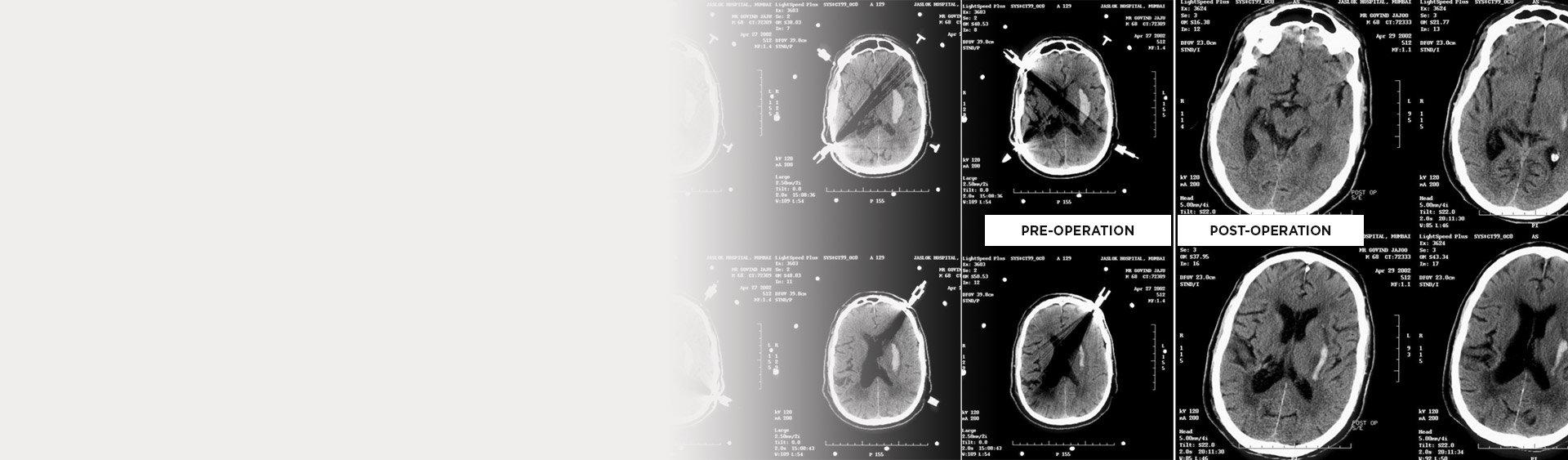
CT scan
- It is the study of choice in acute cases.
- Identification of the location
- Determination of the amount of midline shift
- Detection of hydrocephalus
- Volume estimation of the clot
MRI
- Identifies the cause of haemorrhage
- It is effective in characterizing the age of the haemorrhage
Angiography
- It can be performed if a vascular lesion is highly suspected based on haemorrhage characteristics and location.
Measurement of hematoma volume
The hematoma volumes were determined by CT scan
The CT slice with the largest area of hemorrhage was identified and the volume calculated using, the length ×width × height/2 method.