We perform thalamotomy using CRW Stereotactic apparatus and macro stimulation. The stereotactic frame is fixed to the patient’s head with the help of four pins. The area of fixation is numbed with the help of local anesthetic. The stereotactic frame is placed in a plane parallel to the orbitomeatal line. Following this the patient is taken to the CT scan department where an axial CT scan is performed. The scanner gantry is angled in a plane to include the anterior commissure (AC) and posterior commissure (PC) in one plane
These are fixed landmarks in the brain to which the target can be related. For high degree of accuracy the CT slices are 2mm thick and contiguous. The length of the AC-PC is measured and the thalamic target is chosen as a proportion of this length. It is ½ lateral and 2/10th to 3/10th anterior to the posterior commissure, of the AC-PC length. The relation of the target point to the medial border of the internal capsule is checked and if it is too close or encroaching the medial border than the laterality is adjusted. Once the target is defined the patient is taken back to the operation theatre and made to comfortably lie down on the operation table. A small opening (burr hole) is made in the skull after infiltrating local anesthetic at the operative site. The target is reached with the help of stereotactic arc system.
The physiological exploration is performed using an electrode with an exposed tip of 2 x 2 mm. This is introduced through a precoronal burr hole. The exploration starts 4 mm above the target and the electrode is advanced in increment of 2 mm using micro drive.
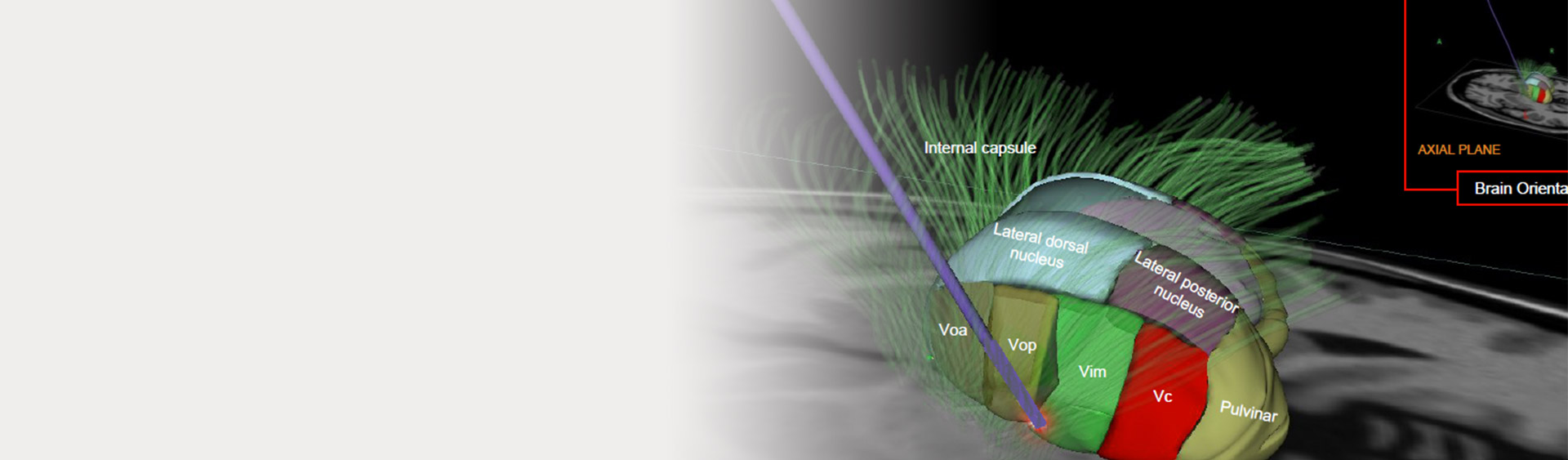
At each level stimulation is performed using 5 Hz. and 100 Hz. frequencies. Motor evaluation to check for weakness, dysarthria and fasciculation’s in tongue is performed at 5 Hz. Sensory evaluations is performed at 100Hz. frequency. During sensory stimulation there is arrest of tremor. The sensory stimulation also guides the laterality of the electrode placement. The topography of the Vim nucleus is corresponding to that of the sensory thalamic nucleus located posterior to it.
The exploration of the final target is continued until one obtains complete arrest of tremors without any side effects. Initially a test lesion of 42 C for 60 seconds is made at this point, and if there is no deficits than a final lesion of 70C for 60 seconds is made. It is important to note that the lesion should not go beyond the AC-PC plane. Thalamic stimulation is performed using similar technique. The advantage of stimulation over lesioning is that it can be performed bilaterally or it can also be offered to a patient with contralateral thalamotomy. It is a useful alternative to thalamotomy in elderly patients.
The morbidity and mortality of thalamic stimulation is less than that of thalamotomy. The side effects are minimal. There are four contact points and innumerable programmable parameters available for programming the electrode. This offers greater flexibility over lesioning in achieving complete tremor control. However, we do not see a role of bilateral thalamic stimulation for PD treatment, as better surgical targets are available. Following the surgery the patient is observed in intensive care unit for 24 hours. In case of thalamic stimulation the IPG (Implantable pulse generator) is implanted on the next day and the programming of the electrode is commenced the day after. The usual hospital stay for thalamotomy is four days, whereas that for the thalamic stimulation is 10 days.
Untoward side effects resulting from a physiologically guided selective Vim thalamotomy are minimal. The most common complications of thalamotomy are pyramidal weakness, dysesthesia, cognitive and speech deficits. The cognitive and speech deficits are more commonly seen in left sided and bilateral thalamotomy. Due to increased incidence of morbidity, bilateral thalamotomy is not performed any more. The risk of intracerebral haemorrhage and infection is less than one per cent.