After a patient gets evaluated on outpatient basis; he / she gets admitted and is thoroughly evaluated by our team comprising of well trained doctors and nurses.
Each individual patient is put through rigorous tests and evaluation parameters which help us to further narrow down the patient’s problems and offer optimum treatment. Routine blood and radiological required for surgery are performed.
The patient is also assessed by anaesthesiologist to determine surgical fitness.
The next day patient undergoes a MRI which may or may not require anaesthesia.
On the day of the surgery the patient is taken to the operation theatre. A frame is fixed to the patients head under local anaesthesia.
Patient is taken for CT scan after frame fixation. After the patient returns from the CT scan his/her head is fixed with the help of the frame to the table. The head is cleaned thoroughly with antiseptic solution.
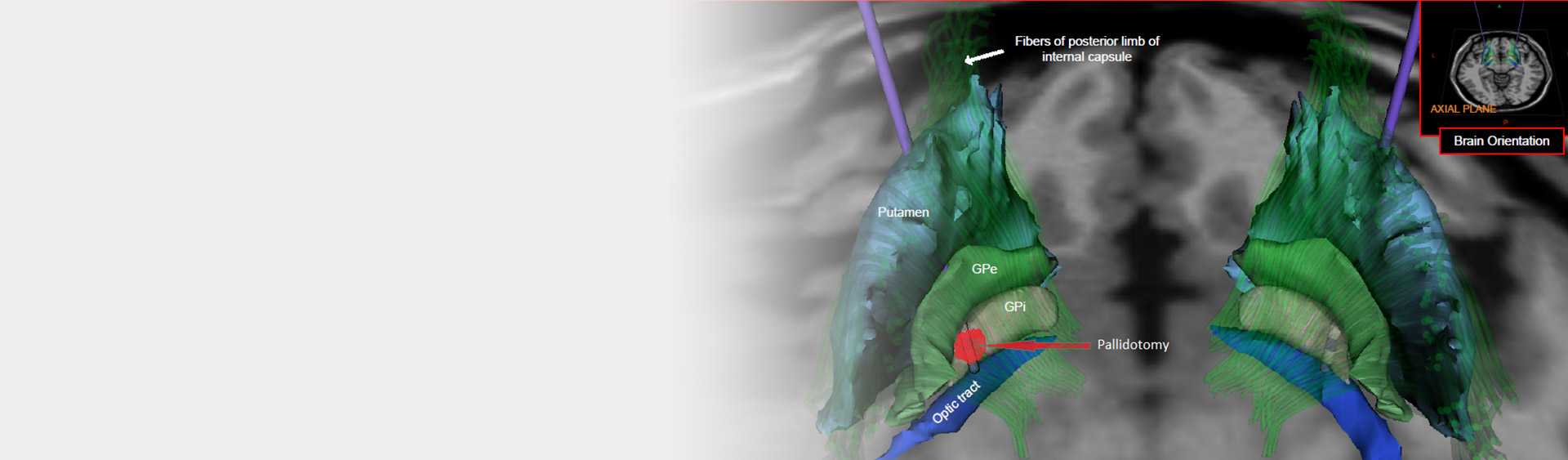
The appropriate surgical trajectory is identified to target the GPi. Incision is taken based on the coordinates under local anaesthesia.
A microelectrode is inserted after creating a small hole in the skull. The electrical recordings are sequentially noted followed by which macro electrode stimulation of target is done during which the patient is assessed for symptom improvement.
A lesion is then created using thermal energy at appropriate level/s. The wound is closed and patient is shifted to CT scan. Patient is subsequently shifted to his/her room.
